
CURE FAQs: Frequently Asked Questions
Answers to commonly asked arterial and metabolic disease questions.
Categories
Click on one of the categories below or type a keyword into the search bar to get started.












Recent FAQs
Statins: The Rest of the Story
You may have heard some of the negative misinformation surrounding statins, which can guide ill informed choices. However, statins are the most effectively proven pharmaceutical treatment for the reduction of heart attack and stroke…
When you are tempted by a podcast influencer sponsored by their proprietary supplement, I suggest that you “follow the money.”
We are being brainwashed by those who prefer that your disease monetize their less reliable and more profitable (for them) supplements or PCSK9 inhibitors or stents and bypass surgery. We modify the use of statins to focus on their beneficial antiinflammatory benefits achieved by using lower doses of safer more effective rosuvastatin.
Our CURE Plans provide optimal outcomes and maximize quality and quantity of life. If antistatinism is your religion, no need to read further. If you suffer from statin derangement syndrome, your resistance will impair our ability to protect you. You won’t be convinced by data or admit you're being fooled. I can’t coach someone who already knows everything, whose ego and stubbornness limit their ability to think critically. Yes, I have a strongly informed opinion on this matter. Unwashing your brain can save your life.
The arguments against statins remind me of the arguments against wearing seatbelts. “What if the car is underwater or on fire and I can’t get the belt off? Wearing it makes me feel uncomfortable.” Today, anyone who doesn’t “buckle up” is deemed foolish in the face of statistics. Yes, we should drive carefully (lifestyle choice) but the seat belt can save us if an accident happens beyond our control. Same with the antiinflammatory protection of statins when inflammation flares due to unanticipated infection (especially dental), trauma, surgery, stress or other events. Or think of statins as fire suppression or a sprinkler system for your arteries.
I'm frustrated when, in addition to prescribing healthier lifestyle and correction of deficiencies, I show the benefits and reversible risks when prescribing statins while monitoring for benefit and harm. Many are stable or improving on well tolerated low dose rosuvastatin. But they stop this life saving treatment in spite of life threatening atherosclerosis with measurable personal improvement in inflammation, arterial age, plaque healing and inflammatory markers because of "something I've read." 🤦♂️🤦♂️🤦♂️
I don’t blame the patient. We are susceptible to “fear porn” propaganda. I blame the opportunists who are pushing people toward far more costly and more profitable PCSK9 inhibitors, expensive and less effective nutraceuticals, stents, surgery, cardiac/stroke rehab, dialysis, memory care centers and funeral expenses in their pursuit of likes, followers, and fees based more on commerce, charisma and charm than interest in your personal outcomes!
Every one of these messengers has a business plan dependent on influencing you!
Everything must be read with a filter of "what is offered as an alternative and what is the conflict of interest?" And "what does the author know or care about my individual circumstances, results and needs?"
I get it, but let’s put facts before feelings on this issue. Are statins mis/over prescribed? For sure. Is it driven by profit motive? This makes no sense. Almost all statins are cheap generics. Just because it is a large industry does not mean it is bad or inappropriate. Far more is spent on food, but we don’t promote starvation.
Mostly, the driver is the guidelines that controlled providers are incentivized to follow and check the box under financial incentives and penalties to adhere. Reducing arterial disease progression or achieving remission doesn’t support a multibillion dollar procedural intervention and rehabilitation business model desiring growth. I’m suspicious of any interventional cardiologist who disputes efforts to achieve remission, including statins. Let’s hear more about the useless and potentially harmful stents placed over the years in asymptomatic individuals provoked by the “oculostenotic reflex” and provider revenue incentives.
Statin fear is used to increase demand for more profitable pharma options like PCSK9 inhibitors (more than $500/month vs $5/month for generic rosuvastatin on GoodRx) and nutraceutical alternatives.
Statins are the most proven pharmaceutical treatment (in addition to a healthy diet and exercise) for remission of arterial disease and the reduction of heart attack and stroke for those with arterial injury/disease/plaque. Drive carefully AND wear your seat belt. Don’t disable the airbag. Don’t light fires, but have a fire extinguisher available if your best efforts fail to prevent the fire.
Evidence strongly supports that statins prevent death and disability from heart attack and stroke in patients with arterial disease. That evidence guides us to recommend statins at lower but still effective and well tolerated doses for those with atherosclerosis, which we identify and measure using carotid ultrasound and coronary calcium scoring. We monitor inflammation levels with ultrasound (intima media thickness measurement) and blood tests: C reactive protein, LpPLA2, microalbumin/creatinine ratio and myeloperoxidase. We consistently see improvement in these measures on statins and deterioration when stopped. I recently documented an 18 year improvement in arterial age in less than 5 months in a 66 year old clean living man while on rosuvastatin 5 mg 3 times weekly in addition to his continued healthy lifestyle. He decided to experiment, stopping the statin. His arterial age returned to the baseline. Now he is a believer. It is common for patients to admit to stopping their statin when confronted with mysterious adverse results on these measures after maintaining they were adherent prior to seeing the numbers. The numbers don’t lie!
You should be far more afraid of untreated inflamed plaque killing or disabling you than concerns about reversible annoying symptoms from an inexpensive generic medication that offers reliable protection. There is little controversy about statin benefit after an event (heart attack, stroke, bypass surgery or stent). When we find plaque (ultrasound or coronary calcium score) we consider those findings as essentially a near miss, an event that, fortunately, did not end in catastrophe. Next time plaque develops, you might not be so lucky.
The foundation of health is nutrition/lifestyle/toxin avoidance. Think of this as the “belt” that keeps our pants from falling down. Statins are like “suspenders” that cover our lapses in optimal lifestyle choices. Safety programs, like airlines and the space program, are built on redundancy and backup plans. Belts AND Suspenders provided by the Department of Redundancy Department. Drive Safely and buckle the Seat Belt! 🙂
Where does the negative information about statins come from?
The biggest problem with statins is higher than needed doses of the wrong statin prescribed for the wrong reason. This is particularly true of the least effective but most effectively marketed statins (e.g. atorvastatin) for the lowering of LDL to target cholesterol levels based on general guidelines. The focus should be on reduced inflammation as measured by LpPLA2, myeloperoxidase and intima media thickness/arterial age by ultrasound in the individual.
At the CureCenter, I don’t prescribe statins if the arteries are healthy, no matter how “bad” the cholesterol is. I prescribe lower doses of rosuvastatin (has shown the strongest evidence of reduction in cardiovascular events while not crossing the blood brain barrier or promoting diabetes) based on documented atherosclerotic arterial plaque or inflammation, identification and monitoring of LpPLA2, myeloperoxidase and carotid intima media thickness/arterial age.
Event risk reduction begins in hours, but not for the reason most think. Statins lower LDL cholesterol levels, but their most potent benefit is reduced inflammation in the artery wall. I have seen this repeatedly by monitoring LpPLA2 and carotid intima media thickness trends.
Statin adherence consistently yields improvement. I can tell when they have been stopped by unfavorable trends in LpPLA2 and CIMT. In other words, they prevent plaque formation, stabilize/heal existing homogeneous and heterogeneous plaque and improve the health and age of diseased arteries! There is evidence they reduced COVID deaths, probably due to suppression of inflammation and mitigating the inflammatory effect of spike protein. Is it possible they protect from vaccine injury as well?
When encountering negative propaganda about statins, ask the following questions:
Is the alternative offered a more expensive and profitable proprietary supplement or pharmaceutical? Statins should cost less than $10/month and are usually covered by insurance. Supplements will cost 2-4 times that amount and not covered by insurance. Ezetimibe is less effective at reducing inflammation. PCSK9 cost more than $500/month. To get coverage, it helps if you are “statin intolerant” which can be promoted by the “nocebo” effect. They cannot claim superior results except with extreme familial hyperlipidemia. But that would make them “orphan drugs. Pharma prefers blockbuster profits.
Does the reduction or elimination of heart attack, stroke, bypass surgery, stents, and rehab for heart attack and stroke undermine their business plan and revenue from treating late stage disease with stents, surgery, rehab, dialysis, memory care centers and funeral expenses?
Is the goal reduction of cholesterol or prevention of heart attack, stroke, premature death, surgery, stents or rehab by suppressing inflammation due to oxidative stress?
Is the advisor using the optimal measurement tools that show improvement in arterial health/age as we do at The CureCenter with Carotid Intima Media Thickness ultrasound or blood markers of arterial inflammation? Or are they solely focused on LDL cholesterol? They need to get with the optimal program, going beyond the standard care guidelines.
Is the advisor like a child with a hammer pounding on everything that looks like a nail? Are they using all the tools and options available from a program in pursuit of optimal quality of life and longevity?
How does the CureCenter prescribe and measure the benefits of statin use?
When prescribing statins, the only reason we monitor lipid levels is that we are expected to do so AND as a way to verify that the medication is being taken. We measure benefit by demonstrating a reduction in measures of inflammation and arterial wall thickness using CIMT.
In some cases, we will pay less attention to elevated cholesterol levels if we know that arteries are healthy based on healthy carotid ultrasound and coronary calcium score.
In other cases, if we know that arteries are sick in spite of normal cholesterol levels, we generally prescribe statins unless we know of prior intolerance based on personal experience. Arteries improve with statins in spite of "normal" cholesterol because statins reduce inflammation. We generally use lower doses (some might say microdoses) of rosuvastatin (fewer side effects) because we are treating for artery health improvement, not the lowest possible LDL cholesterol levels.
Has Dr. Backs had his own personal experience with statin use?
Dr. Backs personally takes a daily statin called rosuvastatin. When he stopped it for a time (to see if his muscles ached from hard workouts or the drug), his arterial age increased by 10 years while he experienced the same sore muscles. This is all while he continued to exercise and live the “cleanest” lifestyle possible. When the statin was resumed, the arterial age returned to lower levels.
Do statins have any side effects?
Statins can provoke dose dependent side effects in a minority of users, most commonly muscle aching. The vast majority of individuals can take them safely with benefit with no adverse results. Untreated sleep apnea and low vitamin D levels increase the likelihood of muscle aches. Correction of these issues reduces these side effects and has other benefits. Coenzyme Q may be helpful, but reducing the dose of the statin or changing to a better tolerated option is the best first step for someone whose arteries are a threat.
A small minority of users have reported cognitive harm in relation to statins. This is less likely with rosuvastatin, our preference, because it does not cross the blood brain barrier like Lipitor/atorvastatin, the most successfully marketed statin that is more likely to raise blood glucose and cause brain fog.
Reduction in arterial disease-related dementia is far greater than the incidence of reversible cognitive compromise from statins. If you experience cognitive changes after starting a statin, they will reverse when the drug is stopped if due to the statin. Don’t get stuck on this worry. Dementia and Alzheimer’s are a far greater risk with arterial disease and insulin resistance driven chronic inflammation. Therefore, addressing this risk is far more important than fearing a temporary side effect.
Increased diabetes risk and insulin resistance have also been a concern. In many cases, patients are not counseled to or fail to reduce sweets and starches in their diets, thinking they are protected by the statin prescription. In fact, the focus on salt, fat and cholesterol leads to increased inflammatory addicting sugar intake. Therefore, it is no wonder that they progress from insulin resistance to prediabetes to Type 2 Diabetes, the progression caused by the western processed glycemic diet. Reduced Sweets, Starches and Snacks in the diet can offset fears about increased risk of diabetes or insulin resistance. Our patients are constantly coached and monitored for evidence of progression to prediabetes or Type 2 Diabetes.
Without personally trying a drug, predicting how you will tolerate it is impossible! The experience of a friend or family member, while provoking understandable concern and fear, will not predict your experience with statins or any other drug. Fears of statin intolerance tend to be self-fulfilling. This is known as the “nocebo” effect.
Intolerance of one statin doesn’t necessarily predict intolerance of all statins. Some side effects disappear with lower doses that will still have benefit measurable by blood and ultrasound measurements of inflammation.
At the CureCenter, we monitor reaction to any medication we recommend, both good and bad. Our bottom line: If you have atherosclerosis, you will generally benefit from a statin (if you can tolerate it) to reverse arterial inflammation, heal plaque and prevent life altering events: heart attack, stroke, and dementia.
If you are still skeptical, we offer alternatives like Bergamot BPF, niacin or red yeast rice, which is chemically a statin. There are other supplements, like nattokinase and turmeric, with claims of efficacy which you can try and see if there is a measurable effect. None of these have the same degree of net favorable track record of statins, and side effects are not zero. They offer benefits that vary by individual.
By the way, statins are a product of nature, like penicillin and antiparasitic/antiviral/antihistamine repurposed meds for COVID and other conditions. Here is Gemini’s AI description:
The history of statins, a class of cholesterol-lowering medications, begins with the discovery of their natural precursors in fungi:
Early Discovery (1970s):2 Japanese scientist Akira Endo at the Sankyo drug company is credited with isolating the first statin, mevastatin (originally known as ML-236B), from the fungus Penicillium citrinum.3 Mevastatin was shown to block the enzyme HMG-CoA reductase, a key step in cholesterol production.4 However, it never reached the market due to concerns over animal toxicity.
First to Market:Lovastatin (Mevacor) was isolated by Alfred Alberts at Merck from the fungus Aspergillus terreus in the late 1970s.5 After initial trials were suspended due to lingering concerns from mevastatin's animal studies, the program was re-initiated. Lovastatin was the first statin approved by the U.S. FDA in 1987, which revolutionized the treatment of high cholesterol.6
The Rise of Synthetic Statins:
Simvastatin (Zocor) was a semi-synthetic derivative of lovastatin, also developed by Merck.7 A pivotal 1994 study demonstrated its effectiveness in reducing cholesterol, heart attacks, and mortality.8
Atorvastatin (Lipitor) was a fully synthetic statin, first patented by Warner-Lambert in 1986 and launched in 1996.9 It proved to be highly potent, and its arrival coincided with an increasing public focus on high cholesterol.10
Blockbuster Status: Atorvastatin (Lipitor) became incredibly popular, and by 2003, it was the best-selling medication in the U.S. and later became the top-selling pharmaceutical of all time [1.1].11
The development of statins was also influenced by other key scientific milestones:
The "Lipid Hypothesis" which linked elevated LDL (bad) cholesterol to coronary heart disease, was increasingly supported by studies like the Framingham study beginning in the 1950s [1.4].12
In 1985, Michael Brown and Joseph Goldstein won the Nobel Prize for their discoveries concerning the regulation of cholesterol metabolism, which provided the scientific foundation for how statins work by increasing LDL receptors [1.2, 1.3].
Open minded willingness to consider risks AND benefits of any treatment leads to the best outcomes. But if your mind is made up, and you decline to take a statin, I won’t “have a stroke” over it.
I hope and pray the same is true for my patients who say “no way” to low dose rosuvastatin.
What tests are done at the CURECenter to measure arterial disease and its root causes?
There is a scientific understanding of the arterial disease (which causes heart attack, stroke and dementia) that is not offered by mainstream medical care. New testing methods and technology enable the CureCenter to offer more individualized and effective treatments…
The true inflammation nature of arterial disease (which causes heart attack, stroke and dementia) is not the model of mainstream medical care. New testing methods and technology enable the CURECenter to offer more individualized and effective treatments.
We offer tests that are not generally available from standard care:
Discover Scan Carotid Ultrasound: This limited low cost carotid ultrasound using point of care Butterfly iQ ultrasound probe and system is like a screening pap smear, mammogram or PSA to detect early cancer. If we find no disease, peace of mind is a benefit. If, however, even a little bit of arterial disease is found (like a little bit of cancer) the images can be sent for a CIMT report (see next paragraph) and then followed to make sure you are safer by following your CurePlan.
Carotid Intima Media Thickness (CIMT) Ultrasound: CIMT measures arterial wall thickness/sickness/inflammation and documents atherosclerotic plaque stage and burden. A thicker artery wall is a more inflamed sicker artery wall. This predicts formation of atherosclerotic plaque and related events such as heart attack and stroke caused by plaque rupture. Arterial wall thickness (inflammation) is more relevant than luminal flow “blockage” in predicting new and unstable plaque formation. Unstable soft or heterogeneous plaque rupture is the event we experience as a heart attack or stroke. This is more likely with new homogeneous unstable plaque. It becomes less likely as plaque becomes more homogeneous/healing and is minimal when plaque is calcified/healed/stable. Proactive optimal care can heal arterial disease and make your arteries healthier and younger with less risk of disability, death or need for rescue procedures.
LpPLA2 (PLAC) Test: This enzyme rises when plaque and artery walls are inflamed or “hot.” You want your arteries to be “cool.” LpPLA2 drops with a less inflammatory diet, exercise, reduced insulin resistance, supplements (niacin, and bergamot and statins. It is a fire alarm or “arterial wall thermometer.”
Myeloperoxidase (MPO): A rise in MPO should trigger a search for neutrophil involved inflammation, especially from the mouth. MPO indicates inflammation and erosion of the inner lining of the artery known as endothelium. A sudden rise should trigger a search for the inflammation that can cause arterial inflammation, leading to heart attack or stroke. Think of a caustic chemical spill inside your arteries. Like a skin abrasion, blood clots form and can occlude flow.
Microalbumin/Creatinine Ratio (MACR): MACR rises most commonly when blood pressure and blood glucose are poorly controlled. This causes dysfunction of the arterial wall endothelium, allowing albumin to leak into the urine in greater amounts. A leaky endothelium fails to protect the intima from processes that lead to inflammation. Think of it as another fire alarm.
For more information about these and other tests, go to
and other information from Cleveland Heart Lab, a major source of our testing
Haptoglobin Genotype: Your Haptoglobin genotype determines if Vitamin E offers protection or increases risk of arterial disease. In addition, individuals with the Hp 2-2 genome are more sensitive to gluten, forming an inflammatory mediator called zonulin that makes your gut “leaky” and raises the risk of autoimmune disease.
Insulin Resistance Testing: Optimally measured through an oral glucose tolerance test, insulin resistance (prediabetes) testing is important in identifying individuals who could be developing vascular complications before a Type 2 Diabetes diagnosis. The glucose tolerance test can identify insulin resistance long before the glucose starts to rise.
However, if there is other evidence of insulin resistance that does not require a visit to the lab, we can skip this step. Clues are seen in levels of nonoptimal HbA1c, glucose, triglycerides above 100, low HDL, and presence of small dense LDL (Pattern B).
The earliest indication for insulin resistance can be measured through body composition testing. We use the InBody 570, a device that can monitor insulin resistance response to changes in diet. Reducing insulin resistance is generally healthy for everyone, regardless of risk.
Continuous Glucose Monitoring (CGM) is now available without a prescription for an affordable $50 for each 2 week sensor. The feedback about individual glucose response to specific food intake provides immediate feedback for diet modification. www.stelo.com
Homocysteine: Elevation increases risk of:
Osteoporosis - bone thinning
Thrombosis (blood clotting)
Heart Attack
Stroke
Dementia
Kidney failure
Neuropathy
Treatment is supplementation with methylated folic acid. Dietary sources of folic acid are leafy greens like spinach and kale. The needed amount of methylated folic acid and Vitamin B12 (and the blood levels) is dependent on the MTHFR gene variant. “Normal” blood levels of folate and B12 are not sufficient for those whose genetics require higher levels for homocysteine safe levels. Therefore, the test we rely upon is the homocysteine level, not the levels of folate or B12. Optimal homocysteine level is less than 8, which may require higher than population norms (yet safe) blood levels of folate and B12.
This paper from the American Heart Association offers a good summary of Homocysteine.
Coronary Artery Calcium Score (CACS): This CT scan detects mature calcified plaque in the coronary arteries. However, it can miss new noncalcified plaque. This test is not useful in monitoring therapy progress/benefit. We recommend CACS when CIMT does not reveal disease but there is still suspicion of coronary artery disease. If this test detects disease that would have otherwise been undetected, a more proactive approach to address root causes will be encouraged. Beware of the slippery slope to a stress test, stents or surgery. Coronary Calcium Score is a “loss leader”for interventional cardiology programs. Call us first before scheduling further tests, especially if you have no symptoms like chest discomfort and breathing issues.
Coronary CT Angiogram with AI Enhancement: This intriguiging advancement should and will eventually largely replace elective coronary angiography. At a cost of $1500+ with radiation and IV contrast associated risk, it isn’t ideal as a screening process. Medicare and insurance coverage is increasing when the alternative is elective catheterization based angiography is the alternative for evaluation of symptoms or heart failure. If money is no object and there is nothing seen on carotid ultrasound focused on the wall (where the action is), it is an option for those who want to go all the way looking under every rock and don’t mind the radiation and contrast risk and inconvenience. The tools don’t fit in a backpack or pocket, that is for sure and they tend to push toward stents and surgery, supporting the “oculostenotic reflex.” For more in depth info, click: https://pmc.ncbi.nlm.nih.gov/articles/PMC9247240/
Home Sleep Testing and Auto Titrated CPAP: These tests have made diagnosis and management of sleep apnea more affordable and effective. Sleep apnea is a root cause of heart attack, stroke, atrial fibrillation, hypertension and heart failure. Treating it can lower your risk of these events, lower your blood pressure, and reduce arterial inflammation.
Oral Microbiome Testing: Oral microbiome testing involves taking a sample of saliva, and analyzing it to identify the types of bacteria present. If high risk bacteria are found, they likely contribute to periodontal and arterial inflammation. In some cases, this can affect management of periodontal disease and contribute to heart attack and stroke risk.
Knowing the occupants of your oral “neighborhood” can prompt a more proactive approach to your oral hygiene. If there are dangerous criminals in your neighborhood, you will be more careful to “lock your doors” and augment your security for protection. The chronic diseases affected by your oral microbiome include periodontal disease, cardiovascular disease, Type 2 Diabetes and prediabetes, and even some cancers and dementia. Options for intervention are best guided by a dentist and hygienist who care about this. General steps include brushing, flossing, water flossing, antiseptic mouthwashes?, oral focused probiotics and xylitol gum. More deeply established infections may require systemic antibiotics and debridement procedures like root planing and deep cleaning followed by maintenance routines.
When is genetic testing important?
Genetic testing should be chosen with an emphasis on tests for which there is a treatment decision that can change the gene expression. Gene expression is the process by which our genes create proteins that perform different functions in our body, such as building and repairing tissues or fighting off infections…
Genetic testing should focus on tests for which there are meaningful remedies that can change the gene expression. Gene expression is the process by which our genes create proteins that perform different functions in our body, such as building and repairing tissues or fighting off infections.
Genetic testing in low-risk individuals with no plan for lifestyle or treatment changes is expensive, confusing and futile.
What genetic tests are most helpful?
Haptoglobin genotype is very worthwhile, especially those with Type 2 Diabetes, insulin resistance, or prediabetes. Most of us fall into one of these categories!
The cost of this test has decreased significantly over the years. In 2018 the test cost about $400. Now, the cost is $99, a small price for precision in personalized treatment. Because it isn’t offered by Quest or Cleveland Heart Lab, we use Boston Heart Diagnostics and provide you their kit to obtain the proper specimen at our office or your home with a dried blood spot card test at an affordable cost of $99 out of pocket. It is not covered by insurance, which might tell you the information can actually improve your health and reduce your costs!
How does haptoglobin genotype guide treatment?
The table below outlines the implications of knowing your haptoglobin genotype.
Haptoglobin Genotype Results and Recommendations
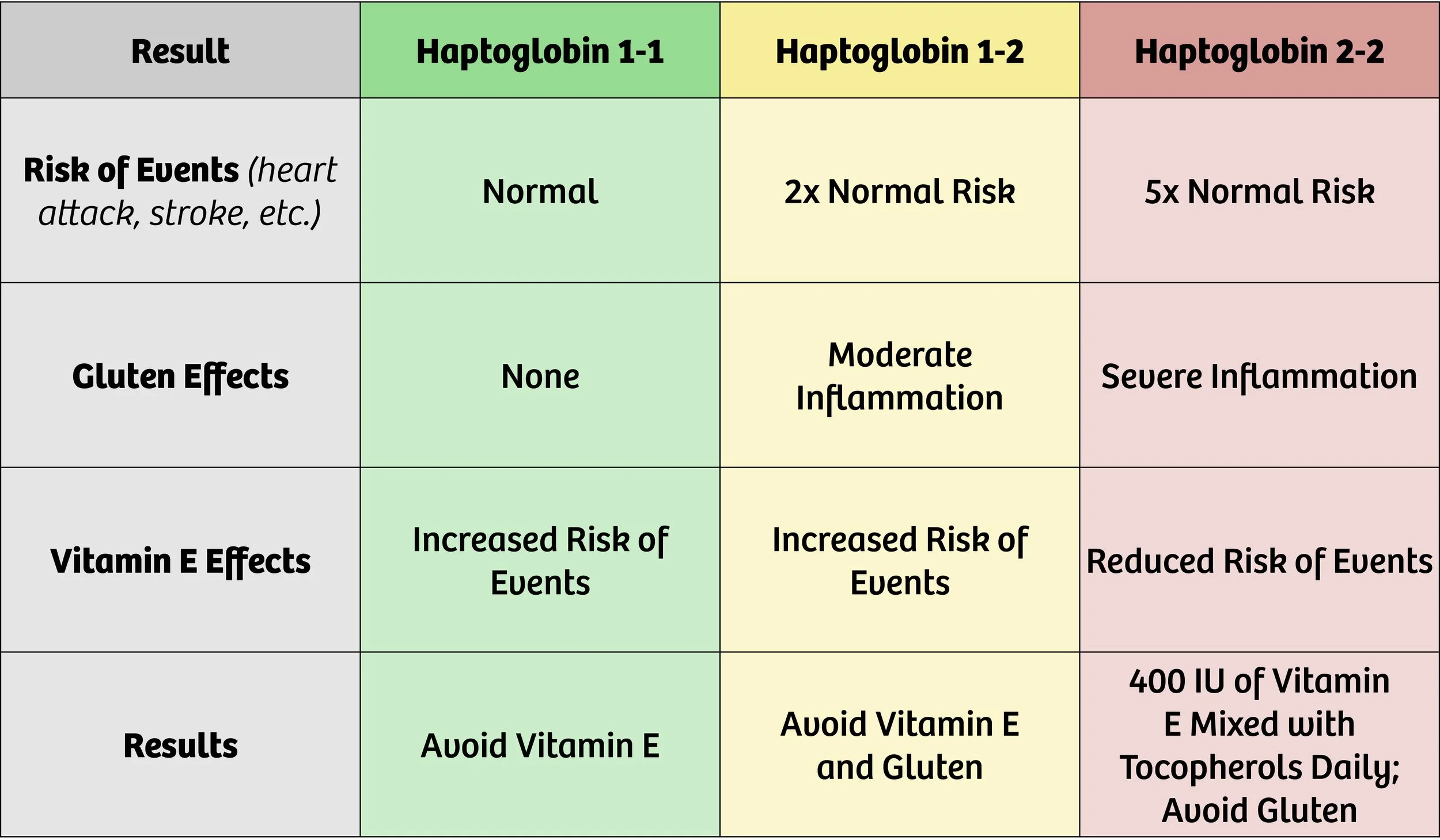
Haptoglobin (Hp) 1-1 is the genotype at the lowest risk for vascular events such as heart attack or stroke. Haptoglobin 1-2 doubles this risk (increases it by 200%). Both of these findings indicate that events are more likely to happen if an individual takes daily vitamin E supplements beyond what is contained in a multivitamin or diet.
Individuals with risk of macular degeneration may be taking supplements containing higher amounts of vitamin E. If your specialist is treating you for current macular degeneration, these supplements make sense. However, you should know that there is a tradeoff. Treating the risk of one condition may increase your risk of another. (See the table above for more information.)
Haptoglobin 2-2 genotype increases risk of vascular events by 500% (or 5x the baseline risk). Gluten should be avoided if this genotype is found, as it provokes a significant increase in inflammation, leading to a higher risk of events.
Individuals with the Haptoglobin 2-2 genotype should take a daily dose of 400 IU of Vitamin E mixed tocopherols to significantlyreduce cardiovascular risk by 80%! The proof is greatest in those with Type 2 Diabetes, but most of us have the prediabetic curse that was a blessing when we ate like hunter gatherers.
ApoE genotype relevance:
We don’t always order ApoE. If you want it, we can order it. In select situations, it can help guide dietary choices, but are less relevant if insulin resistance and carbohydrate restriction is the more compelling opportunity. It often adds more “noise” than “signal.”
The Apolipoprotein E (ApoE) genotype is a genetic factor that plays a significant role in various aspects of human health, particularly in relation to lipid metabolism and the risk of developing certain diseases. The ApoE gene encodes a protein that is involved in the transport and metabolism of lipids, including cholesterol, in the body. There are three common variants or alleles of the ApoE gene: ApoE2, ApoE3, and ApoE4.
The relevance of ApoE genotype lies in its association with several health conditions, including:
Alzheimer's Dementia: The ApoE4 allele is the strongest known genetic risk factor for late-onset Alzheimer's disease (AD). Individuals who inherit one copy of the ApoE4 allele from either parent have an increased risk of developing AD, while those who inherit two copies have an even higher risk. But if you are really interested in reducing your risk of dementia, read “Healthy Heart Healthy Brain” by Bale and Doneen and “The End of Alzheimers” by Dale Bredesen.
Cardiovascular Disease: The ApoE genotype is also linked to the risk of developing cardiovascular diseases such as coronary artery disease and stroke. ApoE4 carriers have been found to have higher levels of LDL cholesterol (often referred to as "bad" cholesterol) and an increased susceptibility to atherosclerosis, a condition characterized by the buildup of plaque in the arteries.
Lipid metabolism: The ApoE genotype influences how the body metabolizes lipids. ApoE2 is associated with lower levels of cholesterol and a reduced risk of cardiovascular disease, while ApoE4 is associated with higher cholesterol levels and an increased risk.
Traumatic brain injury (TBI): Research suggests that the ApoE4 allele may be associated with an increased risk of poorer outcomes following TBI, including a higher likelihood of developing neurodegenerative disorders later in life.
It's important to note that while the ApoE genotype can provide insights into an individual's predisposition to certain conditions, it does not determine with certainty whether someone will develop these diseases. Other genetic and environmental factors generally play a more compelling modifiable role, and individual health outcomes are complex and multifactorial. Genetic testing and counseling can help individuals understand their ApoE genotype and its implications, but it's always best to consult with a healthcare professional for personalized advice and interpretation of genetic information.
KIF6 genotype:
We rarely order the KIF6 genotype. Our preference for rosuvastatin makes it largely irrelevant to guide treatment. If you insist on using atorvastatin, pravastatin or simvastatin, I suggest verifying this is wise based on KIF6 prediction of benefit.
The KIF6 (kinesin-like protein 6) genotype refers to a specific genetic variation in the KIF6 gene. This gene has been studied in relation to cardiovascular health and response to certain medications. However, it is important to note that the current understanding of the relevance of KIF6 genotype is limited, and more research is needed to fully understand its implications.
The KIF6 gene variant in question is known as KIF6 719Arg. It has been associated with an increased risk of coronary artery disease (CAD) and heart attacks in some studies. Individuals who carry this genetic variant may have a higher likelihood of developing these cardiovascular conditions compared to those without the variant.
The KIF6 gene has also been investigated in the context of statin medications, which are commonly prescribed to lower cholesterol levels and reduce the risk of cardiovascular events. Some studies have suggested that individuals with the KIF6 719Arg variant may experience a greater reduction in cardiovascular events when treated with statins compared to those without the variant. However, these findings have not been consistently replicated across all studies.
There is evidence that those with the KIF6 719Arg variant get more benefit from atorvastatin and pravastatin than those not carrying that variant. We prefer rosuvastatin because it is effective regardless of genetic variation and less prone to exacerbate insulin resistance/diabetes or cross the blood brain barrier causing brain fog. Most of our patients take 5 mg 3 days weekly or even less with benefit documented with blood and ultrasound inflammation measures.
It's important to understand that genetic factors, including the KIF6 genotype, are just one piece of the puzzle when it comes to cardiovascular health. Other factors such as lifestyle choices (e.g., diet, exercise), family history, and other genetic variations collectively contribute to an individual's risk for developing cardiovascular conditions.
Overall, while the KIF6 genotype has shown some associations with cardiovascular health and response to statin therapy, its clinical utility is still being explored, and further research is needed to determine its exact relevance and potential implications in healthcare practice.
For more information about genetic testing see our post about genes and how they affect your risk of heart attack.
Get Started on the Path to a Long and Healthy Life

Participate in a 15-30 minute Zoom or phone call with Dr. Backs. Your questions about process, cost, insurance coverage and expectations will be answered. You will decide together if the CureCenter and a CurePlan are right for you.

Located in Central Illinois? Schedule your 15-minute CureScreen for arterial disease. It’s quick, painless, and is the first step toward preventing the most common cause of death and disability.